
.jpg)
.png)
Quick Summary
Behavioral health credentialing diverges sharply from medical: separate payer networks, state-specific Medicaid rules, BH-only license types, and panels that close more often than they open. Most groups wait 60 to 120 days per provider, often stretching past 150 in behavioral health, with weeks of payroll with zero billing. Here’s where the process breaks and how enterprise health systems and growth-stage organizations fix it.
What Is Behavioral Health Credentialing
Behavioral health credentialing is the process of verifying a clinician’s qualifications against primary sources, allowing them to practice and participate in payer networks. The result is a credentialing packet that includes details on license status, board certifications, education, DEA registration, work history, malpractice coverage, and checks for sanctions across OIG, SAM, and state Medicaid exclusion lists.
It’s worth drawing a distinction between credentialing and payer enrollment because the terms are often blurred. Credentialing verifies who the provider is. Payer enrollment is the separate process of adding a credentialed provider to a payer’s in-network roster so that claims can be submitted and paid. A provider can be fully credentialed but may still not be billing if the enrollment process is not yet complete.
BH credentialing follows the same NCQA framework as medical. It includes 11 verification elements, committee review, and recredentialing every two to three years, but the provider types, networks, and state rules diverge enough that generic workflows break down. Credentialing LCSWs, LPCs, LMFTs, BCBAs, psychologists, psychiatrists, and PMHNPs is a different terrain than primary care.
Credentialing vs. Payer Enrollment: Why the Distinction Matters
Operators often use credentialing and payer enrollment interchangeably, but they’re two separate workflows with different stakes.
Credentialing is the verification of who a provider is, what they’re licensed to do, and whether their record is clean across primary sources.
Payer enrollment is contractual, getting that verified provider added to a specific payer’s in-network roster so claims can be submitted and reimbursed.
In behavioral health, the distinction matters more than in primary care. A psychologist can be fully credentialed under PSYPACT and still sit idle for 60 days waiting on enrollment with Optum Behavioral Health or a state Medicaid MCO. Credentialing without enrollment means no billing. Enrollment without credentialing isn’t possible, since payers require a verified file first. Treating them as one process is the most common reason BH groups misjudge their time-to-revenue, especially when expanding into new states or carve-out networks.
Why Listen To Us
We built Assured to credential behavioral health providers faster than any other platform on the market. We’re NCQA-certified as a CVO across all 11 verification elements; we handle BH carve-outs, state-specific Medicaid rules, and ABA workflows. Our customers include BH-focused groups such as Prosper Health and Birches Health, as well as enterprise health systems like Houston Methodist and multi-entity provider groups operating across multiple states. Our customers see 95%+ first-pass approval rates and submissions out within 72 hours of roster handoff.
How Behavioral Health Credentialing Is Different From Medical Credentialing
1. Separate behavioral health payer networks and carve-outs
Most commercial payers handle BH claims through a carve-out rather than their medical network. Optum Behavioral Health, Magellan, Carelon Behavioral Health (formerly Beacon), and Evernorth administer BH networks under their parent plans.
A provider in-network with Cigna for medical care still needs separate credentialing and enrollment for Cigna’s BH carve-out, administered by Evernorth. State Medicaid adds another layer through managed care organizations that contract separately with BH providers.
2. License variety across states and specialties
A medical group credentials MDs, DOs, NPs, and PAs. A BH group credentials psychiatrists, PMHNPs, psychologists, LCSWs, LPCs, LMFTs, BCBAs, RBTs, and peer specialists. A different state board governs each license with a different verification path.
Licensure compacts help in some cases: PSYPACT is live and widely adopted for psychologists. The Counseling Compact launched in 2025 and is operational in a handful of states so far. The Social Work Licensure Compact has been adopted by 30+ states, but isn’t yet issuing multi-state licenses. And MFTs don’t have a compact at all, which means multi-state licensing still requires state-by-state handling for most groups.
3. Medicaid MCO complexity
Medicaid is the largest BH payer in many states. Each state runs its own program, most delegate to MCOs, and every MCO has its own paperwork, panel rules, and timelines. Expanding from Texas into Ohio and Florida means three completely different Medicaid processes, each with its own carve-out and behavioral health rules.
4. Closed panels and the timing problem
BH panels close more often than medical panels, especially in saturated urban markets. Submitting to a closed panel doesn’t fail loudly. It sits in a queue for six to twelve months. Groups that verify panel status before submitting save weeks of wasted cycles.
The Behavioral Health Credentialing Process, Step by Step
Step 1: Gather credentials and documentation
Pull the full provider record, including current state license(s), board certification where applicable, DEA registration for prescribers, malpractice certificate of insurance, NPI, and education transcripts. Get work history for the last five years and any disclosure details. Most delays at this stage come from missing attestations or stale malpractice coverage.
Step 2: Set up and maintain CAQH ProView
Every commercial payer pulls from CAQH. New providers need a profile created, and existing ones need attestations refreshed every 120 days. For BH providers without a CAQH history, common for newly licensed LCSWs, LPCs, and LMFTs, profile creation alone can add three to four weeks.
Step 3: Run primary source verification
Primary source verification is the core of credentialing. Every credential must be confirmed directly with its issuing body, not from copies the provider. For behavioral health providers, PSV covers state licensing boards, education institutions, the NPDB for malpractice history, OIG and SAM exclusion lists, state Medicaid exclusion databases, DEA registration for prescribers, and board certification bodies where applicable.
BH credentialing adds complexity here because a single group may have six or more license types, each verified through a different state board with different turnaround times. Running PSV in parallel across all sources, rather than sequentially, is what separates a two-day turnaround from a six-week one.
Step 4: Compile the committee-ready credentialing file
Once PSV is complete, all verified data is assembled into a credentialing packet. A clean file covers all 11 NCQA verification elements: license verification, education and training, board certification status, DEA registration, malpractice history, attestation content, work history, Medicare and Medicaid sanctions, OIG exclusions, medical board actions, and ongoing sanctions monitoring setup.
For BH providers, this step requires extra attention to license-type-specific documentation. A psychiatrist’s file includes residency verification and DEA records, while an LCSW’s file centers on supervised clinical hours and the MSW degree. Incomplete or mismatched files are the leading cause of credentialing rejections, and each rejection can add 30 or more days to the process.
Step 5: Committee review and credentialing decision
The completed credentialing file goes to the credentialing committee for review. NCQA standards require that a designated committee, which includes a physician or clinical peer, evaluates each provider’s file and makes a formal approve, deny, or defer decision.
The committee reviews the full PSV results, any disclosures or flags, and confirms the provider meets the organization’s or payer’s criteria. For behavioral health, the committee may need to evaluate license types it encounters less often, such as BCBAs or peer specialists, which can slow the review if the committee lacks BH-specific expertise.
A clean, complete file with no open flags typically clears the committee in two to four weeks. Files with disclosures or missing documentation get deferred, adding another cycle.
Step 6: Ongoing monitoring and recredentialing
NCQA standards require continuous monitoring between recredentialing cycles, including monthly OIG and SAM exclusion checks, quarterly license status verification, and tracking of malpractice claims and complaints as they arise.
Recredentialing occurs every 2 to 3 years, depending on the payer, and requires full re-verification of the provider’s credentials. For BH groups, the monitoring burden scales fast: a group with 100 providers across five license types and 15 states has thousands of credential expirations, license renewals, and attestation deadlines to track. Missing a single renewal can trigger a lapse in network participation and halt billing for that provider until the issue is resolved.
How Long Behavioral Health Credentialing Actually Takes
At most organizations, the credentialing process alone takes 30 to 90 days per provider when done manually. Behavioral health groups tend to fall at the longer end of that range because of the variety of licenses, the number of state boards involved, and the frequency of incomplete provider documentation. Here’s how the timeline breaks down:
- Documentation gathering and provider outreach: 1–3 weeks. Provider responsiveness is the biggest variable. Missing malpractice certificates, lapsed attestations, and incomplete work history are the most common holdups for BH providers.
- CAQH profile setup and cleanup: 1–4 weeks. Newly licensed LCSWs, LPCs, and LMFTs without an existing CAQH profile take the longest to obtain. Existing profiles with lapsed 120-day attestations need cleanup before any verification can proceed.
- Primary source verification: 2–6 weeks manually, or 1–2 days with parallel AI-driven verification. State licensing boards are the bottleneck. Some boards respond in 24 hours; others take four to 6 weeks, and BH groups often have 6 or more board types to check per provider.
- Committee-ready file compilation: 1–2 weeks manually, or 1–2 days with automated file assembly. This step involves organizing all PSV results, screenshots, and supporting documents into a single packet covering all 11 NCQA verification elements.
- Committee review and decision: 2–4 weeks. Credentialing committees typically meet on a fixed schedule (monthly or biweekly). Missing the cycle means waiting for the next one. Files with disclosures, malpractice flags, or board actions get deferred for further review, adding another full cycle.
The total end-to-end credentialing timeline, from documentation gathering through committee decision, runs 30 to 90 days for most BH groups doing it manually. With parallel PSV and automated file assembly, credentialing files can be committee-ready in as little as 48 hours once documentation is complete. Recredentialing cycles repeat every two to three years per provider, and each cycle requires a full re-verification of all credentials, not just an update.
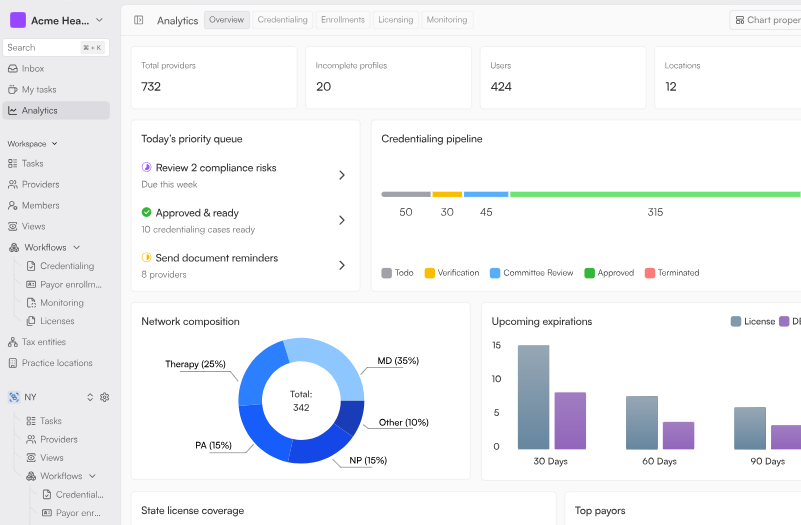
How Behavioral Health Organizations Run Credentialing at Scale
We built Assured because the manual credentialing process breaks the moment a behavioral health organization operates at scale whether that’s an enterprise health system’s BH service line or a multi-state growth-stage network. At 10 providers across two states and three payers, a spreadsheet works. At 200 providers across 30 states and 15 payers, including Medicaid MCOs and BH carve-outs, the spreadsheet is the bottleneck.
Our platform handles the full credentialing lifecycle for every BH provider type. Here’s what that looks like in practice:
- Parallel PSV: AI runs primary source verification across 2,000+ sources in parallel, including state licensing boards, the NPDB, OIG, SAM, state Medicaid exclusions, and education institutions. Credentialing files are committee-ready in 2 business days.
- Payer-specific automation: The system auto-fills applications for Medicaid, Medicare, commercial payers, and BH carve-outs. No portal hopping or manual form entry.
- Medicaid carve-out logic built in: State-specific rules are applied automatically, including separate BH enrollment paths, backdating rules, and MCO requirements.
- ABA workflows: BCBA supervision, RBT requirements, and state-specific ABA credentialing rules handled without manual tracking.
- Continuous monitoring: License expirations, DEA renewals, CAQH re-attestations, and OIG/SAM exclusions tracked daily. Renewals auto-initiated 60 days before expiration.
Our customers see 95%+ first-pass approval rates and submissions out within 72 hours of roster handoff. Birches Health, a behavioral addiction teletherapy provider, reached national network coverage with us in three months.
It onboarded to the platform in under a week, closed 200+ network enrollments, and opened patient access across 40+ states. Their full case study is worth a read if you’re planning a multi-state expansion.
If you’re running BH credentialing on spreadsheets, a legacy vendor, or a point solution that doesn’t handle carve-outs, the math gets hard around 50 providers. The right platform for enterprise health systems and digital health operators alike compresses credentialing from 90–120 days to 30–60 days and keeps it there as operations scale.
Common Mistakes That Delay Behavioral Health Credentialing
1. Incomplete or stale CAQH profiles
CAQH profiles require re-attestation every 120 days. Lapsed attestations invalidate the profile for new applications. Payers can’t pull the data, and the application gets rejected or stuck. New providers without any CAQH history need a profile built from scratch, which adds weeks if it isn’t started early.
2. License and malpractice mismatches
Every payer cross-checks the license and malpractice data on the application against primary sources. A mismatch like expired malpractice by one day, a license renewed in one state but not reflected in CAQH, and an address that doesn’t match NPPES triggers a full re-review. These are the most common reasons for first-pass rejection.
3. Applying to closed panels without checking
Submitting to a closed panel doesn’t produce a clean rejection. The application sits in a queue until the panel reopens, which can take six to twelve months. Verifying panel status before submission saves weeks of credentialing effort on cycles that were never going to close.
4. Slow or missing payer follow-up
Most payers don’t proactively update applicants. Without a five- to seven-day follow-up cadence, applications stall. Groups that assume no news is good news typically discover their applications haven’t moved when they check on day 90.
5. Multi-state licensing gaps
Expanding into a new state without starting the licensing work early adds 60 to 120 days to the credentialing timeline per provider per state. PSYPACT helps for psychologists, but the Counseling Compact and Social Work Licensure Compact are still in early rollout, and MFTs have no compact at all. Most multi-state BH groups still need state-by-state licensing for most of their clinicians.
Scale Credentialing Without Scaling the Chaos
Behavioral health credentialing differs from medical credentialing, and the organizations that handle it cleanly from enterprise health systems with BH service lines to growth-stage multi-state networks treat it as infrastructure rather than an admin task. Carve-outs, Medicaid MCOs, and closed panels change the math at every turn. The right platform compresses the timeline, handles state-specific complexity, and keeps providers billing as operations scale.
To see how quickly your BH providers could be in-network and billing, book a demo now.
FAQ
1. How long does behavioral health credentialing take?
The industry standard is 90 to 120 days per provider per payer, often stretching beyond 150. With parallel PSV and automated submissions, credentialing files can be ready in 2 business days, and applications can be submitted within 72 hours.
2. What’s the difference between behavioral health credentialing and enrollment?
Credentialing verifies a provider’s qualifications against primary sources. Enrollment is the separate process of adding a credentialed provider to a payer’s in-network roster so that claims can be submitted and paid.
3. Do LCSWs, LPCs, and LMFTs need to be credentialed separately from psychiatrists?
Yes. Each license type has its own state board, verification path, and payer-specific rules. Medicare only began covering LMFTs and LPCs in January 2024; psychiatrists have been Medicare-eligible for decades.
4. Can behavioral health providers now enroll with Medicare?
Yes. Marriage and family therapists and mental health counselors became Medicare-eligible on January 1, 2024, under the Consolidated Appropriations Act of 2023. Psychologists, LCSWs, psychiatrists, and PMHNPs were already eligible.
5. How does telehealth affect behavioral health credentialing?
Telehealth doesn’t change credentialing, but it affects enrollment. Most payers reject telehealth-only applications. Providers need a full state license, and enrollment applications should reflect the capability for hybrid practice.
6. Should we outsource behavioral health credentialing or do it in-house?
In-house works for organizations with 10 to 20 providers. Beyond that whether a growth-stage multi-state group or an enterprise health system’s BH service line, the fixed costs of carve-out knowledge, state Medicaid expertise, and monitoring across 2,000+ sources make a managed platform more cost-effective.

.svg)
.png)

