
.svg)
.png)
Quick Summary
Outsourcing payer enrollment can turn months of administrative tasks into a predictable, revenue-protecting workflow, but only if you scope it correctly before signing anything. This guide walks through five practical steps, from auditing your current setup and choosing an outsourcing model to evaluating vendors, planning migration, and managing the partnership.
The Growing Need for Enrollment Support
Every day a provider sits unenrolled is a day they cannot bill. The cost adds up fast. One Assured customer estimated that enrollment delays under their previous vendor cost them millions in lost revenue before they switched.
Payer enrollment contracts providers with commercial plans, Medicare, and Medicaid so that claims are actually paid. It involves maintaining CAQH and PECOS data, submitting payer-specific applications, chasing follow-ups, and staying ahead of revalidations, all while payer rules continue to shift. When a lean internal team tries to keep pace with a growing roster, applications stall and reimbursement slips.
That is why a growing number of healthcare organizations choose to outsource payer enrollment rather than absorb it in-house. This guide breaks down how to do it step by step: what to assess first, how to choose the right partner, and how to keep the engagement accountable.
Why Listen to Us
At Assured, payer enrollment is at the core of what we do. We help enterprise health systems, multi-entity provider groups, and growth-stage healthcare organizations streamline enrollment through automated submissions, CAQH management, and proactive payer follow-ups, making scaling easier.
Birches Health used our platform to onboard providers and get them patient-ready in under a month while expanding across 40 states. That experience gave us firsthand insight into what makes an outsourcing engagement efficient, scalable, and accountable.
Why Outsource Payer Enrollment
Outsourcing comes down to speed, accuracy, and focus. A partner submitting applications every day knows each payer’s submission requirements, current panel status, and escalation paths better than a generalist admin juggling enrollment between other duties.
Cost is the other factor. Building an in-house enrollment team means a salary commitment per specialist plus ongoing training. Turnover in this niche role runs high.. When a single enrollment specialist leaves, institutional knowledge often leaves with them. Outsourcing replaces that fragile dependency with a scalable support that can adapt to changing hiring and growth demands.
For a fuller comparison of the two approaches, see our breakdown of in-house vs. outsourced credentialing. Outsourcing also does not mean losing control. The right partner gives you more visibility into enrollment status than a spreadsheet ever did, not less.
How to Outsource Payer Enrollment Step by Step
Here are the 5 steps to outsource payer enrollment:
Step 1. Get your data foundation clean before anything else
Payer enrollment is a data problem before it is a process problem. Most stalled applications trace back to bad data somewhere. It might be a CAQH attestation that has not been refreshed, an NPPES address that is wrong, an expired liability certificate, or a missing W-9.
Before any partner submits an application, list out every provider, every payer they are enrolled with, every effective date, and every application in progress. Then check the three systems most enrollments depend on:
- CAQH attestations (these expire every 120 days)
- NPPES addresses (they go out of date when providers move)
- PECOS data for providers enrolled with Medicare

When these three do not match, applications stall more often than for any other reason. A good partner spends their first two weeks here. If a vendor wants to start submitting applications on day three, they are skipping the work that decides whether the next 60 days go well.
Step 2. Check panel status before committing to any payer
This is where most enrollment work quietly loses months. When a payer says a panel is "closed," it is a business choice on their end, not a legal rule, and "closed" rarely means closed for everyone.
Check panel status from four sources before you scope the work:
- CMS publishes network adequacy data for Medicare Advantage plans
- State Departments of Insurance publish the same kind of data for commercial networks
- Payer provider directories show when a panel is thin even if the network manager says it is full
- Direct outreach to network managers gives you the real story
When a panel does come back closed, walking away is usually the wrong move.
- File a Letter of Interest addressed to the named network manager.
- Make a Network Gap argument - do you offer something the network does not already have?
Closed panels can reopen anytime, whether a contracted provider leaves, the patient mix shifts, or suddenly there's a slot. Don't wait the six months the rejection notice suggests. Check back every 1 to 2 weeks, because the vendor who checks that week gets in. Florida BCBS and Medicare Advantage plans in busy urban markets are especially prone to this.
Step 3. Choose a partner who can show you the work, not just describe it
Questions about service models are just the starting point. The real scope decisions are payer-specific like commercial only or also Medicare and Medicaid MCOs, individual provider enrollment or also group enrollment, contract negotiation in or out, etc.
Ask to see the working screen during demos where the vendor's team actually does the work, not just the customer-facing dashboard. Bring a real problem from your own provider list and have them solve it on the spot.
Ask three questions:
- What happens when a payer asks for a corrected W-9 on day 45?
- How do you handle a panel that closes mid-submission?
- Can I see your follow-up log for a stalled Optum or UHC application?
Vendors who do this work answer in specifics, and those who don’t fall back to marketing language.
Step 4. Run the engagement on a real follow-up playbook
Follow-up timing matters more than anything else in enrollment. The standard "check in every 14 days" approach wastes weeks.
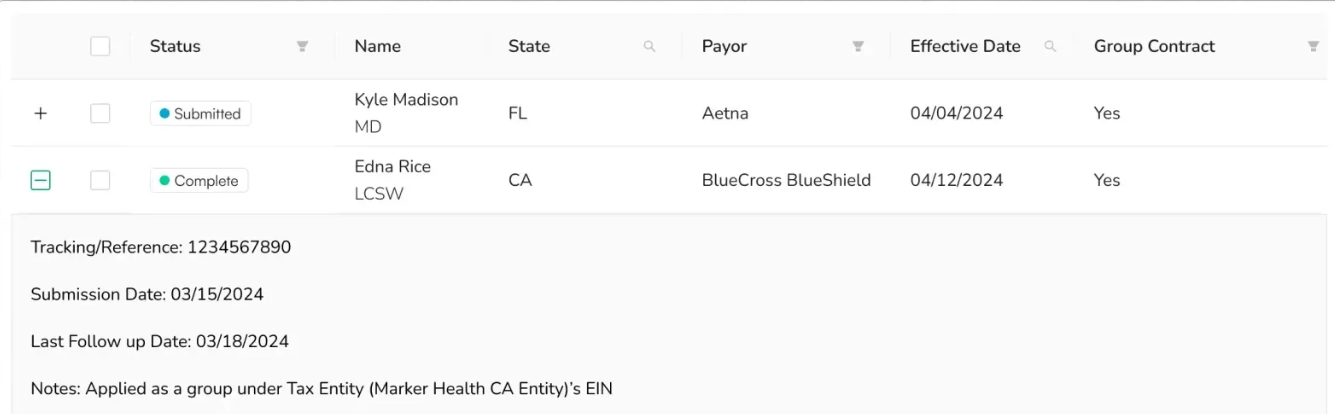
First contact should go out at day 5 to 7 after submission via a phone call and an email. Confirm the payer received the application, obtain a reference number, identify who’s reviewing it, and surface any document requests they haven’t flagged yet. Payers almost never send status updates unprompted. If you’re not asking, your application isn’t moving.
After that, follow up every 10 to 14 days, depending on the payer. Medicare PECOS responds well to a 14-day rhythm. UnitedHealthcare, Aetna, Cigna, and regional BCBS plans move better on 10-day check-ins. Log every call with the date, payer, reference number, rep name, current status, and next action. Without that log, every call starts from zero. Reaching the same coordinator each time also helps, as vendors who build that relationship get faster turnaround.
When follow-up stalls, escalate in steps. No progress at day 30, you can go from your provider rep to a senior rep. On day 45, ask for the network manager. On day 60, you can go to the contracting manager. Every escalation should reference the full log with dates and reference numbers.
For denials, get the exact reason code in writing, fix the specific issue, and resubmit on the same reference number. Resubmitting as a new application restarts your 90-day clock.
Step 5. Build the system that keeps you in-network after approval
Approval is not the finish line.
Medicare revalidates most providers every 5 years under 42 CFR 424.515. State Medicaid programs follow the same 5-year federal floor under 42 CFR 455.414, with some states adding interim attestation requirements on top. You can confirm the specific cycle for every state you operate in.
Commercial recredentialing runs every 36 months under NCQA standards, covering BCBS, UnitedHealthcare, Aetna, Cigna, and others. Start every revalidation at least 60 days before the due date.
Any change, such as a new address, a new state license, or a new TIN affiliation, must be updated in NPPES within 30 days under 45 CFR 162.410(a)(4), and then reported separately to every payer you're contracted with. NPPES updates do not automatically flow to payers.
Check provider directories quarterly. Run sanction and exclusion checks continuously. Miss any of this and a provider can be quietly dropped from a network, which costs the same revenue as never getting enrolled in the first place.
For enterprise health systems and growth-stage organizations, Assured handles the full post-approval lifecycle with revalidation tracking, NPPES updates, directory audits, and continuous monitoring, so your team stays focused on patient care instead of compliance calendars.
Frequently Asked Questions
1. How much does it cost to outsource payer enrollment?
Pricing typically follows either a per-provider fee or a volume-based subscription model, often costing less than hiring a full-time enrollment specialist. Actual cost depends on your payer count and provider mix.
2. How long does the outsourced payer enrollment process take?
A strong enrollment partner can typically submit applications within a few business days of receiving complete documentation. Final approval timelines vary by payer and state, but most average 50 to 60 days, with government plans and closed panels often taking longer.
3. What’s the difference between outsourcing credentialing and outsourcing payer enrollment?
Credentialing verifies who a provider is, covering their licenses, education, and work history. Payer enrollment verifies that the provider is contracted with insurers, so claims get paid. They run in sequence and are often outsourced together, but enrollment is the step that directly unlocks reimbursement.
4. Can an outsourced partner handle Medicare and Medicaid enrollment?
Yes. Most established partners manage commercial, Medicare, and Medicaid enrollment, including state Medicaid MCOs. Government enrollment is more complex and slower, and requirements vary by state.
5. What happens if my outsourced payer enrollment vendor underperforms?
This is exactly why SLAs, reporting, and data ownership matter. If a partner misses agreed-upon benchmarks, your contract should provide a defined escalation path and a clean exit, with your provider data intact.
Choosing a transparent, platform-based partner and seeing the platform before you commit makes underperformance visible early, before it costs you revenue.



.png)
